- CLINICAL PARTICULARS
4.1 Therapeutic indications
ELIGARD 7.5 mg is indicated for the treatment of hormone dependent advanced prostate cancer and for the treatment of high-risk localized and locally advanced hormone dependent prostate cancer in combination with radiotherapy.
4.2 Posology and method of administration
Posology
Adult Males
ELIGARD 7.5 mg should be administered under the direction of a healthcare professional having available the appropriate expertise for monitoring the response to treatment.
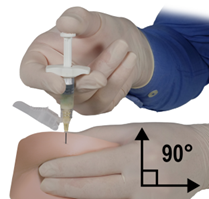
ELIGARD 7.5 mg is administered as a single subcutaneous injection every month. The injected solution forms a solid medicinal product delivery depot and provides continuous release of leuprorelin acetate for one month.
As a rule, therapy of advanced prostate cancer with ELIGARD 7.5 mg entails long-term treatment and therapy should not be discontinued when remission or improvement occurs.
ELIGARD 7.5 mg may be used as neoadjuvant or adjuvant therapy in combination with radiotherapy in high-risk localised and locally advanced prostate cancer.
Response to ELIGARD 7.5 mg should be monitored by clinical parameters and by measuring prostate specific antigen (PSA) serum levels. Clinical studies have shown that testosterone levels increased during the first 3 days of treatment in the majority of non-orchiectomised patients and then decreased to below medical castration levels within 3 – 4 weeks. Once attained, castrate levels were maintained as long as medicinal product therapy continued (<1% testosterone breakthroughs). In case the patient’s response appears to be sub-optimal, it should be confirmed that serum testosterone levels have reached or are remaining at castrate levels. As lack of efficacy may result from incorrect preparation, reconstitution, or administration, testosterone levels should be evaluated in cases of suspected or known handling errors (see section 4.4).
In patients with metastatic castration resistant prostate cancer not surgically castrated receiving a GnRH agonist, such as leuprorelin, and eligible for treatment with androgen biosynthesis inhibitors or androgen receptor inhibitors, treatment with a GnRH agonist may be continued.
Paediatric population
The safety and efficacy of ELIGARD 7.5 mg in children aged 0 to 18 years have not been established (see also section 4.3).
Specific Patient Populations
No clinical studies were performed in patients with either liver or kidney impairment.
Method of administration
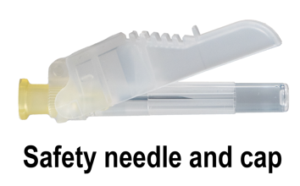
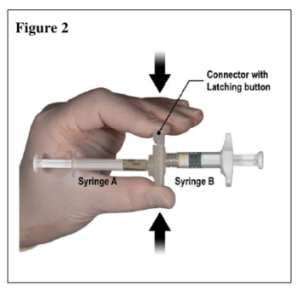
ELIGARD 7.5 mg should be prepared, reconstituted and administered only by healthcare professionals who are familiar with these procedures. Instructions for reconstitution and administration must be strictly followed (see section 4.4 and 6.6.). If the product is not prepared appropriately, it should not be administered.
The contents of the two pre-filled sterile syringes must be mixed immediately prior to administration of ELIGARD 7.5 mg by subcutaneous injection.
Based on data from animal experience, intra-arterial or intravenous injection, respectively, has to be strictly avoided.
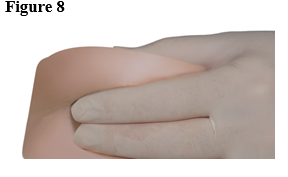
As with other medicinal products administered by subcutaneous injection, the injection site should be varied periodically.
4.3 Contraindications
ELIGARD 7.5 mg is contraindicated in women and in paediatric patients.
Hypersensitivity to leuprorelin acetate, to other GnRH agonists or to any of the excipients listed in section 6.1.
In patients who previously underwent orchiectomy (as with other GnRH agonists, ELIGARD 7.5 mg does not result in further decrease of serum testosterone in case of surgical castration).
As sole treatment in prostate cancer patients with spinal cord compression or evidence of spinal metastases (see also section 4.4)
4.4 Special warnings and precautions for use
Correct reconstitution: Cases of handling errors which can occur during any step of the preparation process, and which could potentially result in lack of efficacy have been reported. Instructions for reconstitution and administration must be strictly followed (see section 6.6). In cases of suspected or known handling error, patients should be monitored appropriately (see section 4.2).
Androgen deprivation therapy may prolong the QT interval:
In patients with a history of or risk factors for QT prolongation and in patients receiving concomitant medicinal products that might prolong the QT interval (see section 4.5) physicians should assess the benefit risk ratio including the potential for Torsade de pointes prior to initiating ELIGARD 7.5 mg.
Cardiovascular diseases: Increased risk of developing myocardial infarction, sudden cardiac death and stroke has been reported in association with use of GnRH agonists in men. The risk appears low based on the reported odds ratios, and should be evaluated carefully along with cardiovascular risk factors when determining a treatment for patients with prostate cancer. Patients receiving GnRH agonists should be monitored for symptoms and signs suggestive of development of cardiovascular disease and be managed according to current clinical practice.
Transient testosterone flare: Leuprorelin acetate, like other GnRH agonists, causes a transient increase in serum concentrations of testosterone, dihydrotestosterone and acid phosphatase during the first week of treatment. Patients may experience worsening of symptoms or onset of new symptoms, including bone pain, neuropathy, haematuria, or ureteral or bladder outlet obstruction (see section 4.8). These symptoms usually subside on continuation of therapy.
Additional administration of an appropriate antiandrogen should be considered beginning 3 days prior to leuprorelin therapy and continuing for the first two to three weeks of treatment. This has been reported to prevent the sequelae of an initial rise in serum testosterone.
Following surgical castration, ELIGARD 7.5 mg does not lead to a further decrease in serum testosterone levels in male patients.
Bone density: Decreased bone density has been reported in the medical literature in men who have had orchiectomy or who have been treated with GnRH agonists (see section 4.8).
Antiandrogen therapy significantly increases the risk for fractures owing to osteoporosis. Only limited data is available on this issue. Fractures owing to osteoporosis were observed in 5% of patients following 22 months of pharmacological androgen deprivation therapy and in 4% of patients following 5 to 10 years of treatment. The risk for fractures owing to osteoporosis is generally higher than the risk for pathological fractures.
Apart from long lasting testosterone deficiency, increased age, smoking and consumption of alcoholic beverages, obesity and insufficient exercise may have an influence on the development of osteoporosis.
Pituitary apoplexy: During post-marketing surveillance, rare cases of pituitary apoplexy (a clinical syndrome secondary to infarction of the pituitary gland) have been reported after the administration of GnRH-agonists, with a majority occurring within 2 weeks of the first dose, and some within the first hour. In these cases, pituitary apoplexy was presented as sudden headache, vomiting, visual changes, ophthalmoplegia, altered mental status, and sometimes cardiovascular collapse. Immediate medical attention is required.
Metabolic changes: Hyperglycemia and an increased risk of developing diabetes have been reported in men receiving GnRH agonists. Hyperglycemia may represent development of diabetes mellitus or worsening of glycemic control in patients with diabetes. Monitor blood glucose and/or glycosylated hemoglobin (HbA1c) periodically in patients receiving a GnRH agonist and manage with current practice for treatment of hyperglycemia or diabetes. Metabolic changes associated with GnRH agonist may also include fatty liver disease.
Convulsions: Post marketing reports of convulsions have been observed in patients on leuprorelin acetate therapy with or without a history of predisposing factors. Convulsions are to be managed according to the current clinical practice.
Idiopathic intracranial hypertension: idiopathic intracranial hypertension (pseudotumor cerebri) has been reported in patients receiving leuprorelin. Patients should be warned for signs and symptoms of idiopathic intracranial hypertension, including severe or recurrent headache, vision disturbances and tinnitus. If idiopathic intracranial hypertension occurs, discontinuation of leuprorelin should be considered.
Severe cutaneous adverse reactions: severe cutaneous adverse reactions (SCARs) including Stevens-Johnson syndrome (SJS), and Toxic epidermal necrolysis (TEN) which can be life-threatening or fatal, have been reported in association with leuprorelin treatment. At the time of prescription patients should be advised of the signs and symptoms and monitored closely for severe skin reactions. If signs and symptoms suggestive of these reactions appear, leuprorelin should be withdrawn immediately and an alternative treatment considered (as appropriate).
Other events: Cases of ureteral obstruction and spinal cord compression, which may contribute to paralysis with or without fatal complications, have been reported with GnRH agonists. If spinal cord compression or renal impairment develops, standard treatment of these complications should be instituted.
Patients with vertebral and/or brain metastases as well as patients with urinary tract obstruction should be closely monitored during the first few weeks of therapy.
4.5 Interaction with other medicinal products and other forms of interaction
No pharmacokinetic drug-drug interaction studies have been performed with ELIGARD 7.5 mg. There have been no reports of any interactions of leuprorelin acetate with other medicinal products.
Since androgen deprivation treatment may prolong the QT interval, the concomitant use of ELIGARD 7.5 mg with medicinal products known to prolong the QT interval or medicinal products able to induce Torsade de pointes such as class IA (e.g. quinidine, disopyramide) or class III (e.g. amiodarone, sotalol, dofetilide, ibutilide) antiarrhythmic medicinal products, methadone, moxifloxacin, antipsychotics, etc. should be carefully evaluated (see section 4.4).
4.6 Fertility, pregnancy and lactation
Not applicable as ELIGARD 7.5 mg is contraindicated in women.
4.7 Effects on ability to drive and use machines
No studies on the effects of ELIGARD 7.5 mg on the ability to drive and use machines have been performed.
The ability to drive and operate machines may be impaired due to fatigue, dizziness and visual disturbances being possible side effects of treatment or resulting from the underlying disease.
4.8 Undesirable effects
Adverse reactions seen with ELIGARD 7.5 mg are mainly subject to the specific pharmacological action of leuprorelin acetate, namely increases and decreases in certain hormone levels. The most commonly reported adverse reactions are hot flashes, nausea, malaise and fatigue and transient local irritation at the site of injection. Mild or moderate hot flashes occur in approximately 58% of patients.
Tabulated list of adverse reactions
The following adverse events were reported during clinical trials with ELIGARD in patients with advanced prostate carcinoma. Adverse events are classified, by frequency, as very common (≥1/10), common (³1/100, <1/10), uncommon (³1/1,000, <1/100), rare (³1/10,000, <1/1,000) and very rare (<1/10,000), not known (cannot be estimated from the available data).
| Table 1: Undesirable effects in clinical studies with Eligard |
| Infections and infestations |
|
| common |
nasopharyngitis |
| uncommon |
urinary tract infection, local skin infection |
| Metabolism and nutrition disorders |
|
| uncommon |
aggravated diabetes mellitus |
| Psychiatric disorders |
|
| uncommon |
abnormal dreams, depression, decreased libido |
| Nervous system disorders |
|
| uncommon |
dizziness, headache, hypoaesthesia, insomnia, taste disturbance, smell disturbance, vertigo |
| rare
not known |
abnormal involuntary movements
idiopathic intracranial hypertension (pseudotumor cerebri) (see section 4.4) |
| Cardiac disorders
not known |
QT prolongation (see sections 4.4 and 4.5) |
| Vascular disorders |
|
| very common |
hot flashes |
| uncommon |
hypertension, hypotension |
| rare |
syncope, collapse |
| Respiratory, thoracic and mediastinal disorders |
|
| uncommon |
rhinorrhoea, dyspnoea |
| not known |
interstitial lung disease |
| Gastrointestinal disorders |
|
| common |
nausea, diarrhoea, gastroenteritis/colitis |
| uncommon |
constipation, dry mouth, dyspepsia, vomiting |
| rare |
flatulence, eructation |
| Skin and subcutaneous tissue disorders |
|
| very common |
ecchymoses, erythema |
| common |
pruritus, night sweats |
| uncommon |
clamminess, increased sweating |
| rare
unknown |
alopecia, skin eruption
Stevens-Johnson syndrome/Toxic Epidermal Necrolysis (SJS/TEN) (see section 4.4), Toxic Skin Eruption, Erythema Multiforme |
| Musculoskeletal and connective tissues disorders |
|
| common |
arthralgia, limb pain, myalgia, rigors, weakness |
| uncommon |
back pain, muscle cramps |
| Renal and urinary disorders |
|
| common |
urinary infrequency, difficulty in micturation, dysuria, nocturia, oliguria |
| uncommon |
bladder spasm, haematuria, aggravated urinary frequency, urinary retention |
| Reproductive system and breast disorders |
|
| common |
breast tenderness, testicular atrophy, testicular pain
infertility, breast hypertrophy, erectile dysfunction, reduced penis size |
| uncommon |
gynaecomastia, impotence, testicular disorder |
| rare |
breast pain |
| General disorders and administration site conditions |
|
| very common |
fatigue, injection site burning, injection site paraesthesia |
| common |
malaise, injection site pain, injection site bruising, injection site stinging |
| uncommon |
injection site pruritus, injection site induration, lethargy, pain, pyrexia |
| rare |
injection site ulceration |
| very rare |
injection site necrosis |
| Blood and lymphatic system disorders |
|
| common |
hematology changes, anaemia |
| Investigations |
|
| common |
increased blood creatinine phosphokinase, prolonged coagulation time |
| uncommon |
increased alanine aminotransferase, increased blood triglycerides, prolonged prothrombin time, increased weight |
Other adverse events which have been reported in general to occur with leuprorelin acetate treatment include peripheral oedema, pulmonary embolism, palpitations, myalgia, muscle weakness, an alteration in the skin sensation, chills, rash, amnesia and visual disturbances. Muscular atrophy has been observed with long term use of products in this class. Infarction of pre-existing pituitary apoplexy has been reported rarely after administration of both short and long acting GnRH agonists. There have been rare reports of thrombocytopenia and leucopenia. Changes in glucose tolerance have been reported.
Convulsions have been reported after GnRH agonist analogue administration (see section 4.4).
Local adverse events reported after injection of ELIGARD 7.5 mg are similar to the local adverse events associated with similar subcutaneously injected products. Generally, these localised adverse events following subcutaneous injection are mild and described as being of brief duration.
Anaphylactic/anaphylactoid reactions have been reported rarely after GnRH agonist analogue administration.
Changes in Bone Density
Decreased bone density has been reported in the medical literature in men who have had orchiectomy or who have been treated with a GnRH analogue. It can be anticipated that long periods of treatment with leuprorelin may show increasing signs of osteoporosis. Regarding the increased risk for fractures owing to osteoporosis (see section 4.4).
Exacerbation of signs and symptoms of the disease
Treatment with leuprorelin acetate can cause exacerbations of signs and symptoms of the disease during the first few weeks. If conditions such as vertebral metastases and/or urinary obstruction or haematuria are aggravated, neurological problems such as weakness and/or paraesthesia of the lower limbs or worsening of urinary symptoms may occur.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance, Website: www.hpra.ie.
4.9 Overdose
ELIGARD 7.5 mg does not have the potential for abuse, and deliberate overdose is unlikely. There are no reports of abuse or overdose having occurred in clinical practice with leuprorelin acetate, but in the event that excessive exposure becomes a reality, observation and symptomatic supportive treatment are recommended.